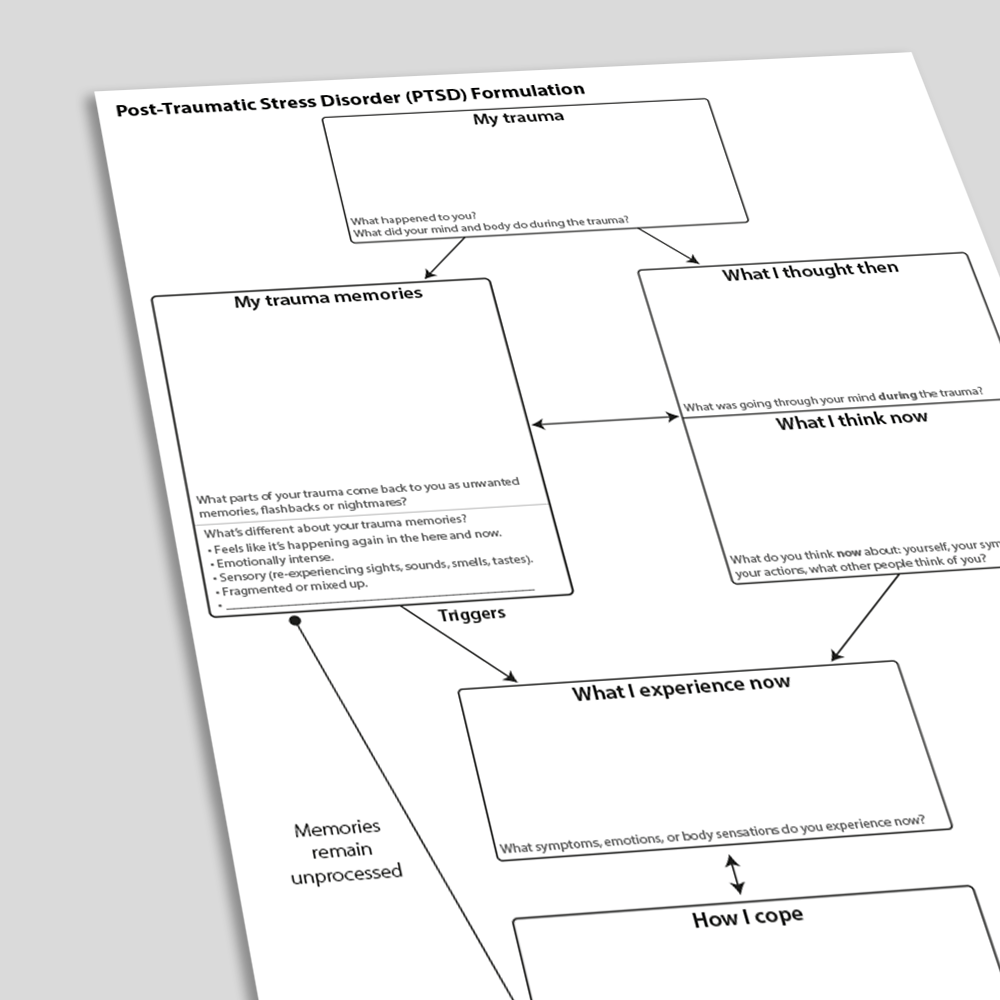
Post-Traumatic Stress Disorder (PTSD) Formulation
This Post-Traumatic Stress Disorder (PTSD) Formulation is designed for use in trauma-focused cognitive therapy for PTSD (CT-PTSD): an empirically supported treatment for post-traumatic stress disorder derived from the Ehlers and Clark model. A crucial early intervention in CT-PTSD is to help clients to develop their own idiosyncratic version of the model, and helping clients to understand how the components of the model maintain their PTSD. This PTSD Formulation worksheet is designed to facilitate this process. It uses client-friendly language, and simplifies elements of the full Ehlers and Clark model in order to help clients to understand what they need at the early stages of therapy.
Download or send

Choose your language
Professional version
Offers theory, guidance, and prompts for mental health professionals. Downloads are in Fillable PDF format where appropriate.
Client version
Includes client-friendly guidance. Downloads are in Fillable PDF format where appropriate.
Editable version (PPT)
An editable Microsoft PowerPoint version of the resource.
Translation Template
Are you a qualified therapist who would like to help with our translation project?
Tags
Languages this resource is available in
Problems this resource might be used to address
Techniques associated with this resource
Mechanisms associated with this resource
Introduction & Theoretical Background
Post-traumatic stress disorder (PTSD) is a common reaction to traumatic events where someone was exposed to actual or threatened death, serious injury, or sexual violence. A large-scale review gave the lifetime incidence of PTSD as 8.3% (Kilpatrick et al, 2013).
Symptoms of PTSD include:
- Intrusion symptoms. These can be characterized by: recurrent, involuntary, intrusive and distressing memories of the traumatic events; recurrent distressing dreams where the content or affect of the dream are related to the traumatic event; dissociative reactions where it feels as though the traumatic events are recurring in the present moment (flashbacks); and intense or prolonged physiological distress at exposure to reminders of the trauma.
- Avoidance symptoms. These might include avoiding or trying to avoid: distressing memories, thoughts, or feelings about the traumatic events; external reminders that trigger distressing memories, thoughts, or feelings about the trauma (e.g., people, places, conversations, activities, objects, or situations).
- Negative
Therapist Guidance
“One of the first steps in cognitive therapy for PTSD is to come to an understanding of what happened to you, how it affected you, and what is getting in the way of your recovery. I wonder if we could explore some of your history, thoughts, feelings, and reactions to see what kind of pattern they follow?”
1. My trauma. The therapist’s role at this point of the formulation is to help the client to briefly label what happened to them. It is important not to probe for too much detail about the trauma at this point, as it may lead to distress, dissociation, or getting sidetracked – the client can be reminded that there will be an opportunity to talk in detail about the trauma during later memory processing. It is helpful at this point to find out whether the client dissociated during the trauma, or if their body
References And Further Reading
- American Psychological Association. (2017). Clinical practice guideline for the treatment of posttraumatic stress disorder (PTSD) in adults. Retrieved from http://www. apa.org/ptsd-guideline/ptsd.pdf
- Brewin, C. R. (2014). Episodic memory, perceptual memory, and their interaction: foundations for a theory of posttraumatic stress disorder. Psychological Bulletin, 140(1), 69.
- Brewin, C. R. (2015). Re-experiencing traumatic events in PTSD: New avenues in research on intrusive memories and flashbacks. European journal of psychotraumatology, 6(1), 27180.
- Ehlers, A., & Clark, D. M. (2000). A cognitive model of posttraumatic stress disorder. Behaviour research and therapy, 38(4), 319-345.
- Ehlers, A., Clark, D. M., Dunmore, E., Jaycox, L., Meadows, E., & Foa, E. B. (1998). Predicting response to exposure treatment in PTSD: The role of mental defeat and alienation. Journal of Traumatic Stress: Official Publication of The International Society for Traumatic Stress Studies, 11(3), 457-471.
- Kilpatrick, D. G., Resnick, H. S., Milanak, M. E., Miller, M. W., Keyes, K. M.,